If your current Near Miss Reporting program feels like a mandatory quota system, you have already guaranteed failure. The goal is not just volume; it is turning those daily “good stories” into structured, actionable data that drives measurable change. This blueprint offers nine systematic moves to fix data quality, increase follow-through, and embed Root Cause Analysis (RCA) into the standard workflow, not the exception. We start with the definition because vague definitions create garbage data.
Near misses are your most powerful leading indicators that reveal where your system will fail before it produces a recordable injury or fatality. Unlike lagging indicators (TRIR, DART, EMR), which measure damage already done, leading indicators like near-miss frequency measure prevention in real time. For a deeper breakdown, see our full guide: Safety Metrics: Leading and Lagging Indicators and Why You Need Both →
1. Eliminate Data Garbage: Define “Near Miss” Precisely
Inconsistent Near Miss Reporting definitions create “definition drift,” making your data useless for trending. A near miss is an unplanned event with potential for injury, damage, or loss, but resulted in none. Distinguish it explicitly from:
- Hazard Observation: A condition (e.g., exposed wire), not an event.
- First Aid Case: An event that resulted in minor harm (injury occurred).
- Property Damage: An event that resulted in equipment or facility loss (damage occurred).
- Unsafe Act: A behavior, not the resulting unplanned event.
Decision Rule: Log the event if it would be reportable had the last variable changed (one inch, one second, one step).
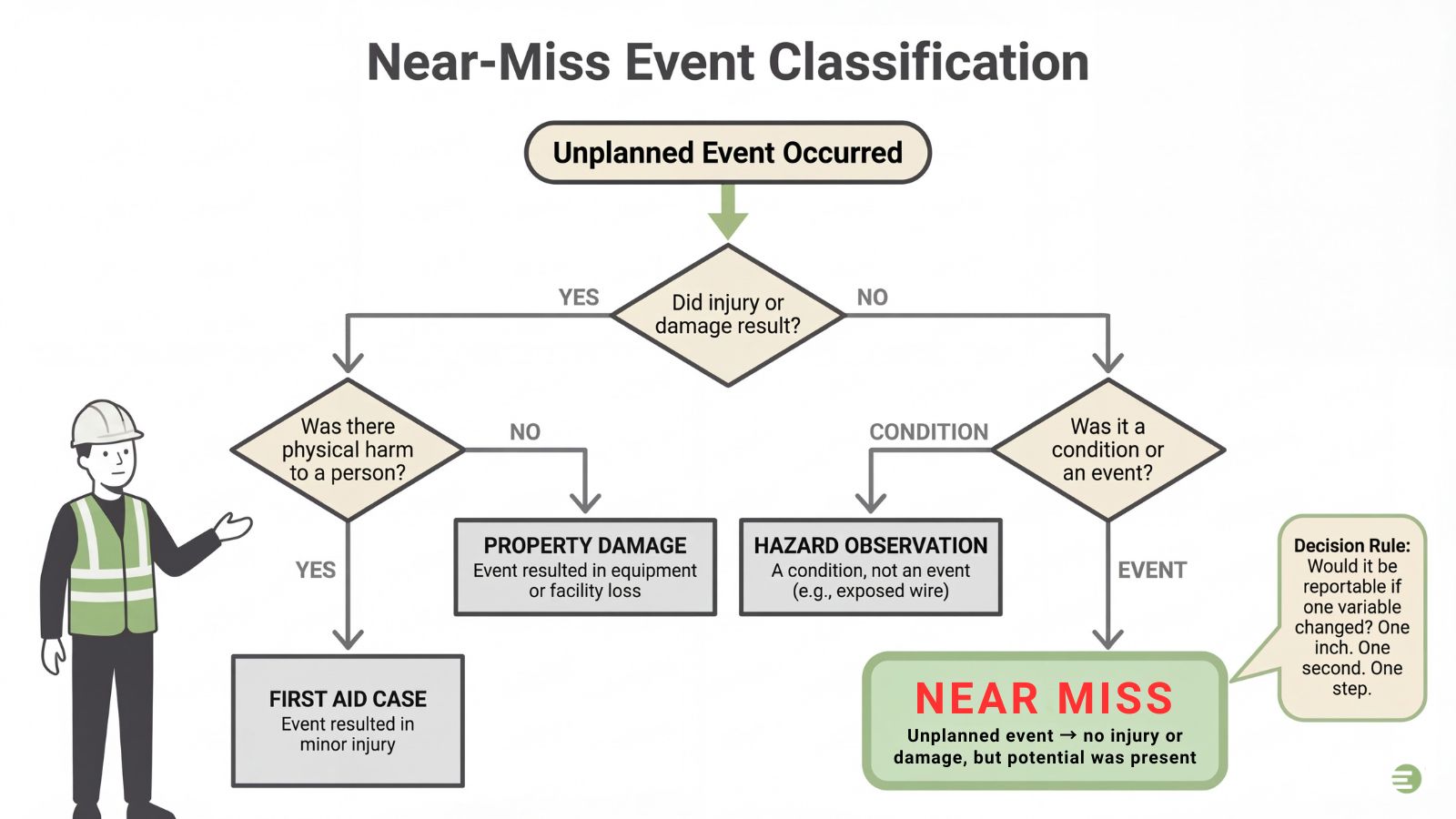
Near-Miss Event Classification
Examples: A dropped construction object that misses the worker; a manufacturing LOTO bypass discovered before equipment energizing; or a chemical splash on a glove, but not skin.
2. Build Credibility: Guarantee Protection for the Reporter
Near miss programs fail when the first reporter is blamed; participation requires a credible “No Surprises” policy guaranteeing psychological safety. This policy requires clear boundaries between protected behavior and actions that trigger discipline:
- Protected: Good-faith reporting, safety observations, and events caused by procedure failure. Anonymity must be guaranteed: investigators review the event data, never the reporter’s identity.
- Unprotected: Intentional harm, sabotage, gross negligence, or impairment on the job.
The manager’s response is the program’s moment of truth. Train leaders to follow this exact script for every report:
- Thank: Express sincere gratitude for the report.
- Ask Two: Ask two non-judgmental clarifying questions (e.g., “Where specifically did this happen?” or “What felt most surprising?”).
- Log & Close: Log the event immediately, explicitly promising a follow-up date for the systemic fix. This follow-through validates the entire program.
3. Minimize Friction: Design a Minimum Viable Reporting System
If your reporting system requires a 10-minute login or 15 fields, you will miss the vital precursors that lead to accidents. Treat near miss reporting like product UX: prioritize speed and ease of use over comprehensive detail. The goal is rapid capture before the employee moves on.
Design a Minimum Viable Report (MVR) requiring only six essential data points: location, time, what happened, what could have happened, a photo/attachment, and immediate action taken (e.g., ‘barrier placed’). For maximum submissions, always make the reporter’s name optional, using a “prefer not to say” option to guarantee anonymity.
To align with jobsite reality, deploy specialized channels: use QR codes linked to offline-capable mobile forms where connectivity is unreliable, or a physical paper dropbox as a non-technical fallback. This streamlined process dramatically increases the volume of high-quality early warning data.
4. Operationalize Actionability: Mandate Systemic Fix Fields
Near miss reports are just noise if they lack structured data for corrective action. To enforce data hygiene, stop collecting vague narratives, and facilitate Root Cause Analysis, mandate these non-optional fields in your reporting template:
- Contributing Factors Checklist: Use forced-choice lists (e.g., Procedure Failure, Equipment Condition, Training Gap) to ensure necessary data points for Root Cause Analysis are collected every time.
- Forced-Choice Control: Implement a dropdown for Recommended Control that aligns directly with the Hierarchy of Controls (Eliminate, Substitute, Engineer, Admin, PPE – aligned with NIOSH’s Hierarchy of Controls). This prevents reporters from suggesting fixes that do not address the systemic root issue.
- Standardized Categories: Use dropdown menus (never open text fields) for high-level demographic data (Site, Crew/Department, Shift, Hazard Type) to ensure all reports are immediately trendable and measurable.
- Mandatory Follow-up: The final field set must include a provisional Owner and Due Date for the corrective action, ensuring accountability for the fix is established at the time of reporting.
5. Establish Triage: Prioritize High-Potential Near Misses
High volume in Near Miss Reporting is useless if low-risk items clog the queue, forcing critical precursors to wait. Implement triage based on potential severity, not just occurrence, to maintain velocity and credibility.
Define a Service Level Agreement (SLA): acknowledge reports within 24 hours, but mandate same-day triage for high-potential events. Use a simple, qualitative Probability × Severity rubric (Low, Moderate, High, Critical) to immediately focus resources on the most dangerous precursors.
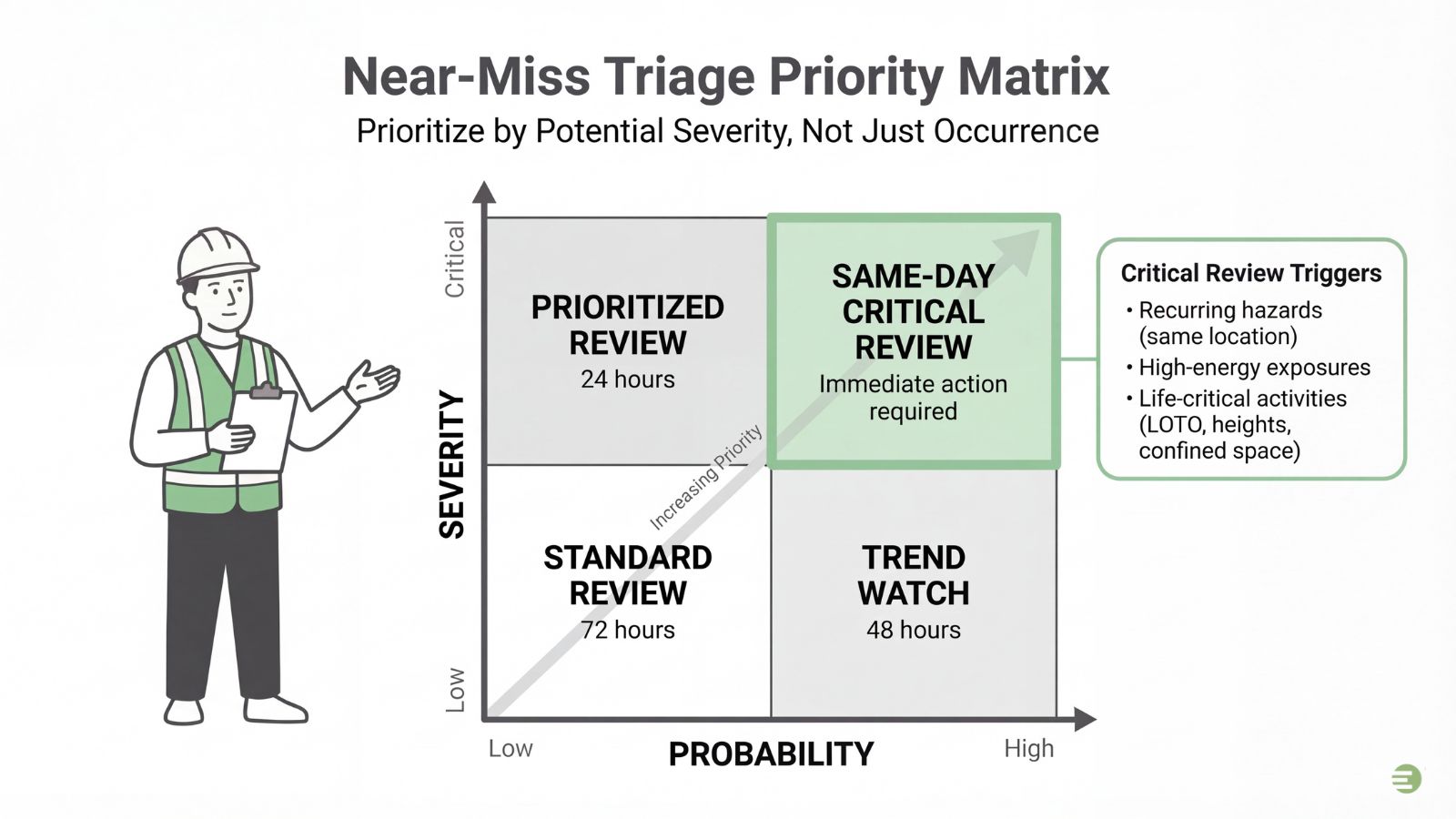
Automatically define the following as critical review triggers:
- Recurring hazards (repeat issues at the same location).
- High-energy exposures (e.g., pressurized systems, electrical faults).
- Near misses involving life-critical activities: line-of-fire, working at height, LOTO bypass, mobile equipment collisions, confined space entry, or uncontained chemical exposure.
6. Standardize Investigations with a Minimum Viable Root Cause Analysis
High-potential events require active Root Cause Analysis (RCA). To ensure repeatability and prevent the “root cause” from becoming a subjective opinion across sites, standardize your investigation minimums:
- Sequence of Events: Document exactly what changed, when, and by whom.
- Conditions Log: Record the environment, equipment, and procedures immediately before the event.
- Witness Check: Verify the sequence with at least one external witness or team member, where possible.
Use a consistent method, like the 5-Whys, to trace the causal chain back to a systemic failure (e.g., Procedure, Training, Design), not an isolated mistake.
Critical Mistakes to Avoid:
- Blaming the Worker: Never let RCA stop at “worker error.” Ask why the mistake occurred (e.g., inadequate training, bad procedure).
- Data Failure: Capture photos or logs before the scene is altered.
- No Owner: Assign a specific Owner and Due Date for implementing corrective actions, ensuring systemic fixes are not abandoned.
- Ignoring the Training Root Cause: When RCA identifies “Training Gap” as a contributing factor, the corrective action must be specific and verifiable, not “retrain the crew.” Browse the full course catalog →
7. Close the Loop: Mandate Concrete Corrective Actions
Near-miss programs fail when corrective actions are superficial (e.g., reminders or unread SOPs). To force systemic fixes and maintain credibility, the workflow must demand a measurable result before the case is closed.
Every reported incident must mandate one of these three outcomes:
- Assigned Permanent Control: A systemic fix (e.g., engineering control) with a clear owner and due date.
- Immediate Temporary Control: A rapid mitigation (e.g., temporary barrier, equipment shutdown) alongside a mandated permanent plan.
- Documented Rationale: A written justification for zero action, reserved for extremely rare cases.
Prioritize Elimination or Engineering controls over simple Administrative fixes or PPE. To truly close the loop, require concrete evidence of completion: a photo of the installed guard, the updated SOP, or a purchase order for new equipment. No evidence, no closure.
8. The Credibility Lever: Close the Feedback Loop, Publicly
If Near Miss Reporting submissions vanish, trust and future participation dies immediately. Credibility is the highest leverage point for sustainable engagement. Implement a highly visible feedback loop using two core practices to ensure every report yields a measurable outcome.
- Response Guarantee: Every non-anonymous submission requires a direct, three-part response: thank you, status, and scheduled next step. For anonymous reports, respond publicly via a weekly “Good Catches” board or toolbox talk slide. Always focus the disclosure entirely on the hazard and fix, never the individuals involved.
- Trend Dissemination Cadence: Allocate five minutes weekly to share data ROI during toolbox talks. Report the top three hazards identified and the three biggest corrective actions completed. Use this analysis to link directly to relevant refresher [construction training resources] or update SOPs, proving that reporting drives operational change.
9. Monetize the Precursors: Frame Near Miss ROI for the C-Suite
Translate near-miss data into executive finance language. Presenting “reduction in incident likelihood” secures no budget; quantifying “avoided $500k in equipment downtime and claims costs” does. Data must predict and quantify savings.
Position control implementation as a measurable ROI. Use historical incident costs to quantify systemic fixes as avoided costs against that average. Run a focused 90-day pilot; success provides the proof required for scaling. For centralized training and multi-site administration, explore our Business Accounts →
The 30-Day Near Miss Program Execution Schedule
Operational failure often occurs in the handoff from strategy to implementation. Programs stagnate when organizations fail to define “who does what by when.” This 30-day schedule minimizes dependencies, moving you from collecting reports (Item #3) to enforcing systemic corrective actions (Item #7) rapidly.
Prerequisites: Adopt the precise definition of a near miss (Item #1) and select your minimum viable reporting (MVR) intake channel (Item #3) before starting Week 1.
Week 1: Foundation and Policy Lock-In
The focus is psychological safety and clarity.
- Define: Roll out the precise definition of a near miss (Item #1). Use examples to clarify the distinction between a hazard and a precursor event.
- Trust: Write and publish the non-punitive safety policy (Item #2), detailing protected behavior boundaries.
- Configure: Set up the MVR form (Item #3). Integrate systemic fix fields (Item #4) to mandate categories and control recommendations.
Week 2: Launch and Data Inflow
The focus shifts to rapid deployment and manager buy-in.
- Deploy: Launch the MVR channel across all sites, including quick-access QR codes.
- Train: Conduct mandatory supervisor briefing (Item #2) on the “Thank, Ask Two, Log & Close” response script.
- Announce: Publicly announce the feedback guarantee timeline (Item #8), promising follow-up on reported fixes.
Week 3: Triage and Systemic Analysis
The focus is transforming raw reports into actionable priorities.
- Prioritize: Implement the Triage SLA (Item #5). Flag high-potential reports for immediate review based on energy exposure and recurrence.
- Investigate: Mandate the 5-Whys (Item #6) for all high-risk events to search for systemic failures, not human error.
- Review: Start reviewing early trends (Item #9). Identify the top three reported factors or locations for the first public update.
Week 4: Closure and ROI Quantification
The focus is accountability, completion, and proving program value.
- Accountability: Enforce documentation (e.g., photo, updated SOP) as required evidence before officially closing any case (Item #7).
- Publish: Publish the first high-visibility “Good Catches & Systemic Fixes” update (Item #8) to build credibility.
- Quantify: Use new data to quantify avoided risk (Item #9), framing implemented controls as measurable ROI for executive review.
Outcome: At the 30-day mark, the system must produce measurable data, enforce action closure, and shift the operation from reactive management to proactive risk reduction.
Frequently Asked Questions (FAQs)
1. What is a near miss (near miss meaning)?
A near miss is an unplanned event where contact, damage, or injury was narrowly avoided. It is often described using the “one inch, one second, one step” rule: if one of those variables had changed, a severe incident would have occurred. A near miss is distinct from a hazard observation (a condition) or an incident (an event resulting in actual damage or injury). Your program must capture the potential, not the outcome.
2. What are near miss examples in construction or manufacturing?
In high-risk environments, near misses are precursors to fatalities. Common examples include a dropped hammer falling past a worker on a scaffold (struck-by); a power tool guard jamming before the operator makes contact (caught-in/between); an employee walking through an unsecured LOTO boundary before the machinery is energized; or a pressurized hose detaching and spraying steam away from personnel (high-energy exposure).
3. Does OSHA require near-miss reporting?
OSHA does not explicitly mandate internal near-miss reporting or tracking, as these are considered leading indicators and are often non-recordable events. OSHA’s compliance focus is strictly on recordable injuries and reportable events (fatalities, amputations, in-patient hospitalizations). However, internal company policies or large client contracts frequently mandate robust near-miss programs as evidence of proactive risk management.
Additionally, OSHA’s Voluntary Protection Programs (VPP) explicitly require participants to investigate all near misses and maintain written investigation reports as a core element of their safety and health management system (OSHA VPP Policies and Procedures Manual, CSP 03-01-005). OSHA’s own Recommended Practices for Safety and Health Programs also identify near-miss reporting as a fundamental component of effective worksite analysis. Organizations pursuing ISO 45001 certification or alignment with ANSI/ASSP Z10 will find that both frameworks mandate hazard identification processes that include near-miss capture and corrective action tracking as baseline requirements.
4. How do we stop people from submitting “fake” near misses for rewards?
Design your recognition system to reward quality of action, not raw volume. Never offer per-report cash incentives. Instead, focus on team-based recognition, rewarding the groups that successfully close systemic actions, identify the most dangerous precursors (high-potential catches), or reduce the Repeat-Near-Miss Rate. This strategy validates the process and prevents gaming the system with low-value submissions.
5. Should we use paper forms, spreadsheets, or EHS software?
If your goal is systemic change, you will quickly outgrow spreadsheets. For rapid, high-volume near-miss reporting, use mobile-first EHS software or dedicated apps. These tools handle offline submissions, enforce mandatory follow-up fields (Owner, Due Date), guarantee anonymous submission options, and automatically generate the dashboards required for executive-level ROI reporting (See Item #9 above).
6. How long should we retain near-miss records?
While OSHA’s recordkeeping standard (29 CFR 1904.33) mandates a five-year retention period for OSHA 300 Logs and 301 Incident Reports, near-miss records are not covered by this specific regulation because they are non-recordable events. However, best practice is to retain all near-miss reports, investigation findings, and corrective action documentation for a minimum of five years, mirroring the OSHA recordkeeping retention period. Many organizations retain them longer for legal defensibility, audit readiness, insurance documentation, and long-term trend analysis. If your organization operates under ISO 45001 or ANSI/ASSP Z10, your management system documentation requirements may dictate specific retention schedules—consult your registrar or legal counsel for guidance.
Sources: OSHA, NIOSH